
EDITOR’S SUMMARY: Grasping the true significance of MMR vaccination goes beyond the familiar pro-vax vs. anti-vax debate. As today’s health landscape differs vastly from the pre-vaccine era, it’s crucial to explore the nuances of vaccine-induced versus natural immunity to truly understand the far-reaching implications of both.
By Verity Bell
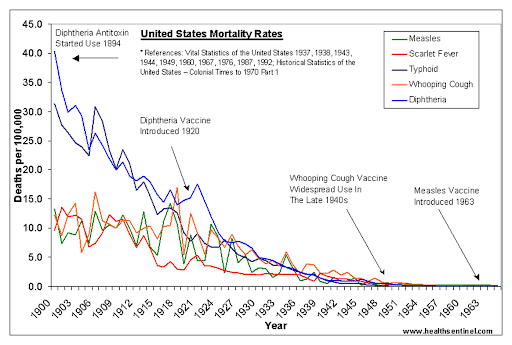
In recent years, growing skepticism has exposed cracks in the prevailing narrative around vaccination. While publicly acknowledging risks and harms has cost doctors their reputations and careers, the mismatch between vaccine myth and the historical record has long been an open secret. As most recently confirmed by the study, “Annual Summary of Vital Statistics: Trends in the Health of Americans During the 20th Century,” the sharp declines in death from infectious disease in the first half of the century preceded the introduction of most vaccines. Contrary to widely held beliefs, these declines resulted from improvements in nutrition, sanitation, and social conditions.
Many people have begun to suspect that vaccination may, in the words of Robert Mendelsohn, M.D., from his 1984 book, “How to Raise a Healthy Child in Spite of Your Doctor,” “be responsible for the dramatic increase in autoimmune diseases, cancer, leukemia, rheumatoid arthritis, Lou Gehrig’s Disease, lupus, and Guillain-Barré syndrome.” Have we, as Mendelsohn concluded by asking, “traded mumps and measles for cancer and leukemia?” The sharp rise in autism alongside the rapid expansion of the vaccine schedule has only heightened parental concerns, despite ongoing efforts by the government and pharmaceutical industry to deny any connection. Lately, vaxxed-unvaxxed studies have emerged, including those by Joy Garner, Brian Hooker with Neil Miller, and Paul Thomas, M.D., with James Lyons-Weiler. These studies suggest that the unvaccinated are significantly healthier, suffering less not only from autism, but also from attention-deficit/hyperactivity disorder (ADHD), asthma, allergies, developmental or learning disabilities, and other chronic conditions.
The appointment of Robert F. Kennedy, Jr. as head of the United States Department of Health and Human Services has inspired hope in many individuals that greater transparency and independent research will shed light on some of these potentially troubling connections. Assuming this were to transpire, and the majority were to decide that vaccine-induced immunity was not worth the health risks, what would the implications be? Would the transition back to natural immunity be an easy one or might there be some hurdles along the way? And if there were hurdles, what would be the most effective way to navigate them? This article will focus on measles, mumps, and rubella to address these questions. There is no doubt that reclaiming natural immunity would have benefits. It is longer lasting than immunity induced by vaccines (in some cases, permanent), and considerably more broad spectrum (protective against a wider range of viral strains). Moreover, as Richard Moskowitz, M.D. points out in “Vaccines: A reappraisal,” overcoming febrile infectious illnesses in childhood strengthens the innate immune system, greatly reducing your likelihood of developing numerous forms of cancer in later life. It also protects against the following:
“… asthma, allergies, seizures, and a variety of autoimmune disorders, including type 1 or insulin-dependent diabetes mellitus (IDDM), idiopathic thrombocytopenic purpura (ITP), Crohn’s disease, ulcerative colitis, and even coronary artery disease.”
Moskowitz goes so far as to postulate that contracting infections naturally is essential for expelling pathogens from the blood. He suggests that introducing them in a way that bypasses the mechanisms of the innate immune system could cause them to remain in the organs, potentially triggering autoimmunity and inflammation. All this notwithstanding, to the extent that vaccination has reduced the prevalence of infection, it is worth exploring what its abandonment might mean in the short term. Vaccine injury, as debilitating, potentially fatal, and staggeringly under-reported as it may be, is not the only consequence of injection. Replacing natural immunity with a weaker, less durable alternative has shifted infections to age groups that are more vulnerable to severe illness and complications. Take measles, for example, an illness in which the groups at greatest risk of complications are adults and infants.
Prior to the introduction of the first measles vaccine in 1963, these groups were largely shielded since nearly everyone contracted the virus as a child, leaving them with lifelong immunity. Infants less than a year old were rarely infected because naturally-immune mothers transferred antibodies and lymphocytes to their babies via the placenta and through breastfeeding (a protection that vaccinated mothers are unable to confer to the same degree). Consequently, according to research compiled by Neil Miller in his Vaccine Safety Manual, from 1960–1964, only 10% of cases occurred in children over 10, whereas by 1977 this had shifted to 60%, and as much as 78% during a 1978 outbreak in Rhode Island. Likewise, by 1992, 28% of cases occurred in infants under a year—to whom measles vaccines are not given, as they are not effective. If vaccination were to decline and infection rates were to rise, what would the risk profile look like without these protective demographic buffers?
Physicians for Informed Consent (PIC) estimate that the death rate from measles in the pre-vaccine era was 1 in 10,000 in the U.S. While this figure differs from the higher rate of 1 in 1,000 that is often quoted, it is based on blood tests indicating that nearly everyone contracted measles, which (given the population at the time) suggests that 90% of cases went unreported. One of the most serious side effects of measles is encephalitis (brain swelling), of which 25% of cases (1 in 80,000 or 0.00125%) lead to neurological injury, such as developmental disability, deafness, or blindness, and occur at an overall rate of 1 in 20,000 (0.01%). Arguably the most severe—but also the rarest—is a condition called Subacute Sclerosing Panencephalitis (SSPE), a progressive and generally fatal neurological disease with a delayed onset of up to several years. It occurs at a rate of 6 to 22 per million (0.0006–0.0022%). Other complications include pneumonia, seizures, ear infections, fever, diarrhea, and dehydration. These conditions, regardless of their rarity, are undeniably alarming, and often serve as a key argument for vaccination. What is less often considered or discussed is that all of these issues are also listed in the package insert as adverse events of the Measles, Mumps, and Rubella (MMR) vaccine. Moreover, they are accompanied by numerous repercussions, including disorders like transverse myelitis, Guillain-Barré syndrome, thrombocytopenia, meningitis, pancreatitis, diabetes, and arthritis, among others.
In fact, PIC found the risk of seizures from the MMR (potentially resulting in permanent harm) to be five times higher than that from natural infection. Given the under-reporting factor for vaccine-related complications, which the Lazarus study suggests could be higher than 99%, an accurate comparative risk profile would not be easy to establish. For context, the last recorded measles death in the U.S. was in 2015, when a vaccinated woman who was taking immunosuppressive medications for other serious health conditions passed away. Since then, two more deaths have been reported in the media, but it remains unclear whether the adult and child died from measles itself or merely had the virus at the time of death due to unrelated causes. Conversely, as stated in an article by the National Vaccine Information Center (NVIC), “Side Effects of the Measles Vaccine Include Brain Damage and Death”:
“As of November 30, 2018, there have been more than 93,179 reports of measles vaccine reactions, hospitalizations, injuries and deaths following measles vaccinations made to the federal Vaccine Adverse Events Reporting System (VAERS), including 459 related deaths, 6,936 hospitalizations, and 1,748 related disabilities.”

Can You Trust Your Natural Immunity?
To return to the question of risks posed by the virus itself, if a large portion of the population were to stop vaccinating, would the rate of fatality and adverse outcomes be higher than in the pre-vaccine era? Assuming there were to be a resurgence of infection, this is certainly a possibility. An article by Children’s Health Defense, “Natural Measles Immunity — Better Protection and More Long-Term Benefits Than Vaccines,” noted that researchers in Sicily and France found adults to be almost twice as likely as children to experience complications. It also cited a 2017 measles outbreak in Italy, where 73.8% of cases (n = 3,301) occurred in people over the age of 15. Not surprisingly, as revealed in a Lancet study, this demographic shift has led to a 4.5 times higher rate of serious issues from measles.
That said, it’s unclear whether a resurgence would be an inevitable result of ceasing vaccination, as disease incidence may not always be directly linked to vaccine uptake. There were, for instance, no measles cases documented in the unvaccinated Amish community of Lebanon County, Pennsylvania, over a 17-year period from 1970 to 1987. The MMR vaccine initially reduced the incidence of the illnesses it targeted, but the extent to which it continues to do so remains uncertain. For example, outbreaks have been documented in communities with 99% and 100% vaccine compliance, suggesting that either the vaccine’s efficacy was more limited to begin with than claimed, or that it had waned. Diminishing immunity can happen in some cases, in fact, in as little as 10 years, and attempts to boost it through revaccination have proven ineffective. There is even evidence linking a significant proportion of cases during outbreaks to the vaccine-strain virus.
The media, in deference to its pharmaceutical sponsors, consistently blames epidemics on the unvaccinated. In the 2015 Disneyland outbreak, which led to the repeal of California’s personal belief exemption (by way of SB277), 30% of cases were later found to involve the vaccine strain (either induced by vaccination, or transmitted by vaccinated individuals through viral shedding). Additionally, 31% of cases occurred in individuals who could prove they had been vaccinated. The percentage of vaccinated cases may have been even higher, given that 20 of the 131 cases with unconfirmed vaccine status were adults who self-reported receiving the vaccine. This, coupled with the fact that viral shedding from live vaccines can persist for over 100 days, suggests that vaccination campaigns may be perpetuating cycles of outbreaks. For these reasons, from “The Future Of Measles In Highly Immunized Populations: A Modeling Approach,”a computer model simulation predicts that by 2050, susceptibility could exceed pre-vaccine levels, even if vaccine uptake remains high. The crucial issue, then, is how you can mitigate your risk, whether you choose to vaccinate or not. Fortunately, one indisputable fact is the connection between disease outcomes and nutritional status. According to the authors of “Nutritional Risk, Micronutrient Status and Clinical Outcomes: A Prospective Observational Study in an Infectious Disease Clinic”:
“Malnutrition is the most common cause of immunodeficiency worldwide and probably causes a significant percent of deaths from infectious diseases in developing countries.”
As Suzanne Humphries M.D. and Roman Bystrianyk, authors of “Dissolving Illusions: Disease, Vaccines, and The Forgotten History,” encouragingly remark:
“In the developed world today, where good nutrition is possible,
where vitamin A is readily accessible just about everywhere, where
knowledge about supporting a healthy immune system is available,
there is no reason to have encephalitis of any sort, or for anyone to
go blind with measles.”
In the chapter on measles, Dr. Humphries explains how the key to healthy recovery from measles lies with the function of the innate (or cellular) arm of the immune system, which is contingent upon dietary nutrition. This is different from the more measurable humoral (antibody-mediated) immunity, which is the main focus of vaccinology. The fact that people who cannot produce antibodies still recover well from measles highlights the importance of this immunity. As Humphries points out, the overstimulation or artificial administration of antibodies can interfere with the immune system’s innate ability to clear the virus. This interference has been linked to the development of cancer and autoimmune diseases. This was seen both in children who were vaccinated while they still had maternal antibodies, and those injected with immunoglobulin. These children failed to develop the signature measles rash, which Humphries describes as evidence of the “cell-mediated reaction” on the part of the innate immune system that kills infected cells. This absence of rash was similarly observed in cases of Subacute Sclerosing Panencephalitis (SSPE), which Humphries attributes to “incomplete viral clearance,” and which was reported in one study to have increased in incidence since vaccination. In connecting these dots, Humphries echoes the concern expressed by Moskowitz, that bypassing the mechanisms of innate immunity may cause more serious problems by “trapping measles virus in the body.” Instead, she says it should “be met with a cellular immune system replete with vitamins A, C, and D.”

Perspective, Treatment, and Recovery
With an emphasis on vaccination, treatment options are often overlooked, but doctors in Texas have had success treating cases in the recent outbreak using cod liver oil, the steroid budesonide, and the antibiotic clarithromycin. Vitamin A is included in the Centers for Disease Control and Prevention’s (CDC) recommendations for measles treatment. Its therapeutic value is linked to the virus’s tendency to deplete vitamin A in the body. It protects the eyes, supports the immune system in preventing viral replication, and significantly reduces mortality. Vitamins C and D contribute by protecting against the potential complications of opportunistic bacterial infections, such as pneumonia and otitis media (ear infection). Cod liver oil is a potent supplemental source of vitamins A and D, as well as omega-3 fatty acids. Foods high in vitamin A include beef and chicken liver, fish, eggs, and dairy. It can be obtained to a lesser extent from orange and yellow vegetables and dark leafy greens, although these forms are less bioavailable. Notably, the healthiest sources of vitamin C come from organic foods like acerola cherry and camu camu, rather than synthetic ascorbic acid.
Mumps and rubella, the other viruses targeted by the MMR vaccine, are both benign when contracted in childhood, and confer permanent immunity (as well as protection against ovarian cancer in the case of mumps). However, when contracted after puberty, mumps and rubella can lead to more serious problems, such as infertility in males or fetal damage in pregnant females. Additionally, as with measles, vaccination has resulted in higher incidence rates in this age group. The symptoms for rubella, as documented by Physicians for Informed Consent (PIC), involve no more than a head to foot rash for children in the 50% of cases that are symptomatic, preceded by cold symptoms in adults. Deaths from contracting the virus after birth are extremely rare, occurring in about 1 in 210,000 cases (0.0005%). The greater risk is Congenital Rubella Syndrome, which affects certain fetuses when a woman contracts the virus during the first trimester. This condition occurs in about 1 in 29,000 cases (0.0035%) and can lead to death or lifelong disabilities for the baby. Ironically, since the introduction of the vaccine has led to more cases of rubella in post-pubescent girls, this complication, as revealed in the aforementioned Lancet study, has increased by 5.8 times.
According to PIC, “Mumps – Disease Information Statement (DIS),”symptoms—when present (in 73–85% of cases)—include:
“… muscle pain, loss of appetite, fatigue, headache, low-grade fever, and swelling of the parotid glands (located on the sides of the face, between the ear and jaw).”
The most severe complications could lead to hearing impairment (1 in 360,000 or 0.0003%), fertility impairment in post-pubescent males (1 in 290,000 or 0.0004%), or death (1 in 93,000 or 0.001%). Unfortunately, as they also note, a quarter of children lose protection from mumps in 7.9 years after MMR, and a third lose protection from rubella after 15 years. As a result, most mumps outbreaks in recent years have occurred in vaccinated college students. Here are several measures you can take to protect yourself and your loved ones from mumps, measles, and rubella. Since the body’s first line of defense against infectious illness is your innate immune system, the most important thing you can do is support it with a healthy lifestyle. This means getting sunlight (and/or infrared light from other sources) daily, sleeping well, engaging in regular physical activity, eating organic, unprocessed foods, and limiting exposure to toxins, whether from the environment or personal care/home products, and reducing exposure to electromagnetic fields (EMFs)—cell phones, computers, Wi-Fi routers, smart meters, microwave ovens, and other electrical appliances. An essential component of immunity is nurturing your gut with prebiotics, probiotics, and postbiotics, as your digestive tract houses 70% of the immune system. Herbal remedies such as elderberry and nigella sativa (black seed) can also help.
Consistent with the observations of Drs. Moskowitz and Humphries, a critical factor in supporting your innate immune system is to refrain from interfering with its functioning. If you or your child come down with a fever, for example, suppressing it with medication like acetaminophen (Tylenol) may not be the best course of action. As explained by Jennifer Wolff-Gillispie in her article, “Fevers: To Cool or Not to Cool … That Is the Question,” acetaminophen reduces the glutathione in the body that is needed for detoxification. She goes on to point out that fever is a mechanism employed by the immune system to kill the pathogen it is combating, while minimizing collateral damage. For infants under one month old with a fever, or those under three months with a fever exceeding 100°F, medical advice may be needed if they appear lethargic, confused, or have pronounced abdominal pain. At this age, they have not yet developed the ability to self-regulate their temperature. Since fevers from infection rarely exceed 105°F and will not generally result in brain damage below 107°F, focusing on hydration is the most effective way to facilitate optimal recovery in most cases.
Although society may have been better off if natural immunity had not been undermined by vaccinations, transitioning back to it now could come with substantial risks. Given the erosion of durable natural immunity, it seems reasonable to assume that with a decline in vaccination, the viruses they target would become more prevalent. This would likely be a necessary step to re-acquire natural immunity, but the severity of the illnesses may also increase. Realistically, it is probable that there would be a greater number of severe cases than in the 1960s, not only because more vulnerable age groups are now susceptible (including infants), but also because the population’s baseline level of health has deteriorated dramatically since then. In fact, the rate of chronic illness has risen from 12% in the 1980s to between 50% and 56% in older adults as of 2021. An increasing number of doctors are questioning whether the growing vaccine schedule may have contributed to this rise, possibly due to incomplete clearance of the injected viruses.
Regardless of the validity of these concerns, the establishment continues to promote a single narrative: “vaccines are safe and effective” and “measles can kill.” This creates a significant barrier to exercising your right to informed consent, due to underlying conflicts of interest. Critical thinking, on the other hand, calls for weighing the risks of any virus against the potential for injury or harm from the vaccine. Whichever side you lean toward, avoiding complications from infection will likely depend as much on what you embrace as on what you reject. In other words, if you decide to turn away from the conventional approach of vaccination, symptom suppression, and routine antibiotics, having a clear sense of what you plan to do instead is key. It may be worth collaborating with a naturopathic doctor who offers integrative treatments, such as intravenous high-dose vitamin C, glutathione, and B vitamins, as well as herbal medicine. Additionally, committing to a diet of unprocessed, organic whole foods, staying active daily—whether through simple yoga practices or other movements—and keeping natural remedies on hand can further support your health. So called “vaccine-preventable” diseases may ultimately be less preventable than vaccine advocates would have you believe. However, your body has an incredible, innate ability to fight illness. By making proactive, health-promoting choices, you can significantly boost your chances of robustly bouncing back.
~
Published on March 13, 2025.
If you’ve found value in this article, please share it!
To support the research and health education of AVFC editorial, please consider making a donation today. Thank you.